VERVE‑102 is a Phase‑1 trial that uses CRISPR base editing to inactivate PCSK9 in liver cells with a single injection — a one‑and‑done strategy intended to lower LDL for years. This piece pulls the available trial details, explains why the approach mirrors natural PCSK9 loss‑of‑function found in a small fraction of people, and — crucially — lays out the unresolved safety, regulatory and access questions that mean statins aren’t going away anytime soon.
Key Takeaways
- VERVE-102 uses CRISPR base editing to permanently disable the PCSK9 gene, potentially providing lifelong cholesterol reduction from a single treatment.
- The approach mimics natural genetic mutations found in 1-3% of people who have 15-40% lower LDL cholesterol and reduced heart disease risk throughout their lives.
- While promising, this Phase 1 trial focuses on safety rather than efficacy, and statins remain the proven first-line treatment with decades of safety data.
What Makes VERVE-102 Different from Current Treatments
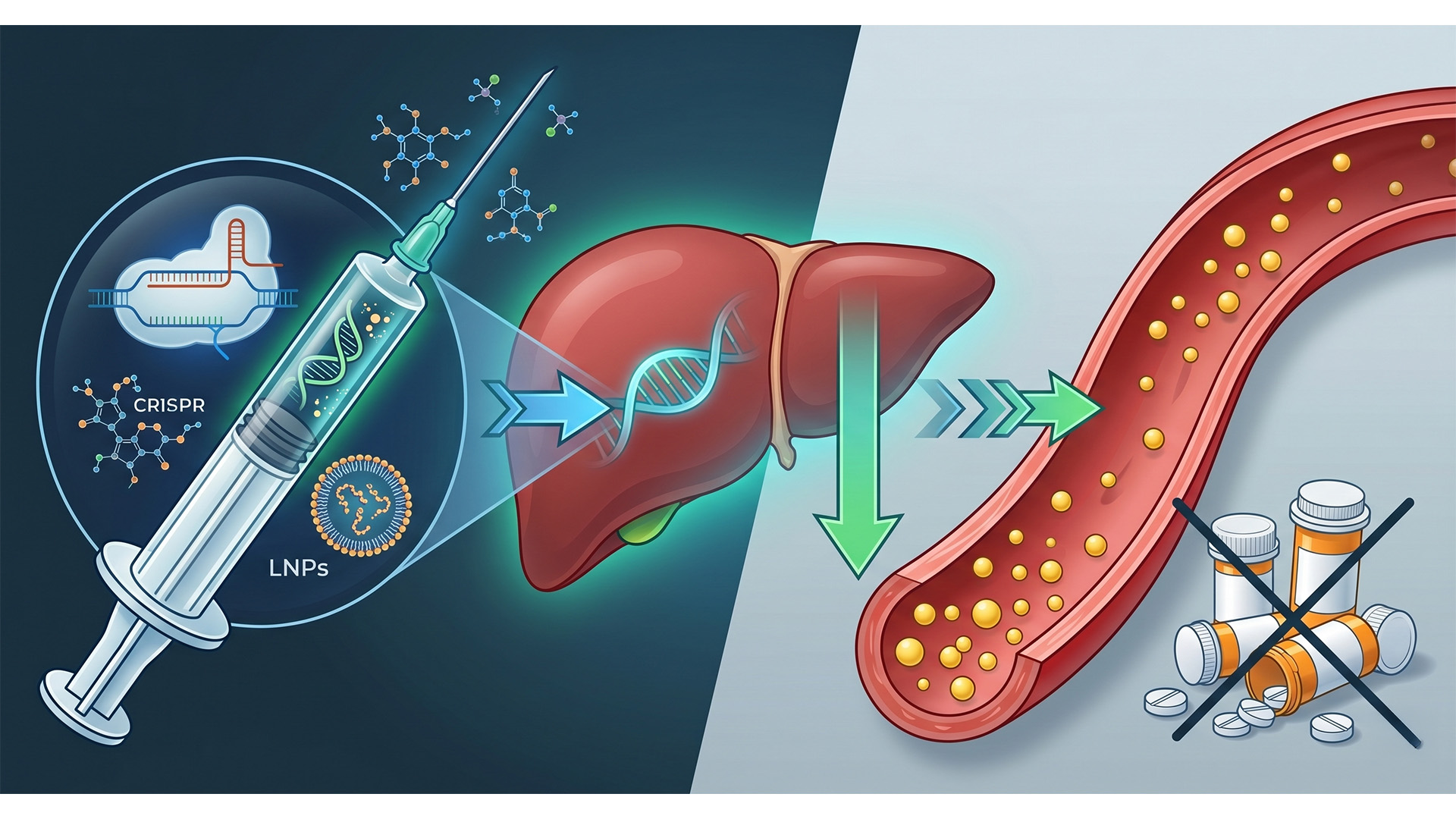
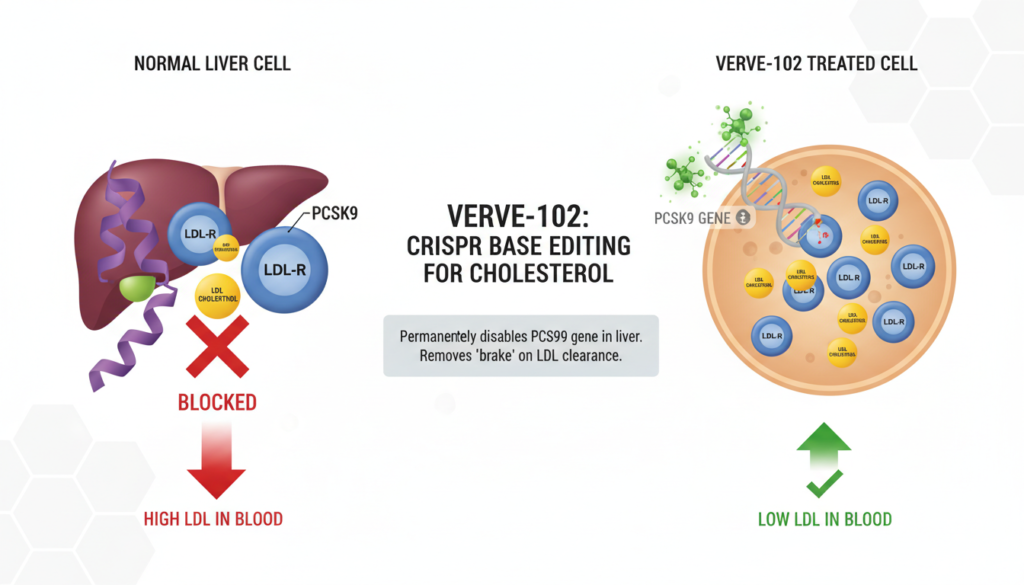
VERVE-102 uses CRISPR base editing to permanently disable a single gene in your liver called PCSK9. This protein normally acts like a brake on your liver’s ability to clear LDL cholesterol from your blood. By turning off this brake, your liver becomes more efficient at removing harmful cholesterol.
The treatment involves injecting lipid nanoparticles containing the gene-editing components directly into participants. Think of it as a molecular delivery system that carries genetic scissors specifically to liver cells. Unlike daily statin pills, this approach aims to provide permanent cholesterol reduction from a single treatment.
What makes this particularly compelling is that it mimics something nature already does. About 1 to 3% of people are born with mutations that reduce PCSK9 function. These individuals enjoy 15 to 40% lower LDL cholesterol throughout their lives and significantly reduced heart disease risk, with no apparent negative effects.
Early Results Show Promise, But Limited Data Available
Initial results from the first cohort demonstrate meaningful reductions in LDL cholesterol. However, complete data remains limited as this is an ongoing Phase 1 trial focused primarily on safety rather than efficacy. The company has been appropriately cautious about releasing detailed numbers, which is standard practice for early-stage studies.
The theoretical advantage is significant: unlike daily medications, gene editing could provide lifelong effects from a single treatment. The edited genes would be passed down to daughter cells as liver cells naturally regenerate over time, maintaining the cholesterol-lowering effect indefinitely.
But you need to understand what Phase 1 actually means. This isn’t about proving the treatment works better than existing options - it’s about determining whether the approach is safe enough to warrant larger studies. Efficacy questions come later.
Why Statins Remain the Gold Standard
Despite the excitement around gene editing, statins have decades of safety data in millions of patients. They reduce cardiovascular events by approximately 20 to 25% and are generally well-tolerated across diverse populations.
More importantly, if you experience side effects from a statin, you can simply stop taking it. With gene editing, you cannot easily reverse the changes. This represents a fundamentally different risk profile that many patients and doctors will need to carefully consider.
Current evidence suggests PCSK9 inhibition is safe based on genetic studies of people with natural mutations and from injectable PCSK9 inhibitor drugs like evolocumab. However, permanent genetic modification carries theoretical risks that may not manifest for years or decades.
The Cost and Accessibility Factor
Personalised genetic therapies typically carry substantial price tags initially, potentially limiting accessibility compared to generic statins that cost pennies per day. Even if VERVE-102 proves effective, the economic reality may restrict its use to specific high-risk populations for years to come.
Real Safety Concerns That Need Addressing
Gene editing faces several hurdles that pharmaceutical drugs don’t encounter. Off-target effects represent a primary concern - situations where the editing occurs at unintended sites in the genome. While CRISPR base editing is more precise than earlier techniques, it’s not 100% specific.
Immune responses to the delivery system itself pose another challenge. Your immune system might recognise and attack the lipid nanoparticles, potentially reducing effectiveness or causing unwanted reactions.
The trial requires careful screening and is limited to specific patient populations. We’re not discussing a treatment that would be broadly available anytime soon, even if the results prove overwhelmingly positive.
Where Gene Editing Might Actually Fit
Rather than replacing statins entirely, VERVE-102 might serve as a complementary option for specific situations. Consider patients who cannot tolerate any statin despite trying multiple formulations and dosing strategies. Or individuals with extremely high cardiovascular risk who need every possible intervention to prevent heart attacks and strokes.
The research represents promising but early-stage science. Larger safety and efficacy studies are needed before any potential clinical application becomes reality. You’re looking at years, not months, before this could reach routine clinical practice.
For most patients managing cholesterol, statins will likely remain the primary treatment for the foreseeable future. They work, they’re proven safe, and they’re widely accessible. The infrastructure for prescribing, monitoring, and adjusting statin therapy is well-established in healthcare systems globally.
The Bottom Line on Gene Editing for Cholesterol
Gene editing in medicine is advancing rapidly, but it’s crucial to separate genuine scientific progress from sensationalised headlines. VERVE-102 represents an intriguing approach that could eventually provide an additional tool for cardiovascular disease prevention.
However, calling this “the end of statins” significantly overstates where the technology currently stands. Statins remain the proven, accessible first-line treatment for most people requiring cholesterol management. Any future role for gene editing would likely complement, rather than completely replace, existing proven therapies.
The most realistic scenario involves gene editing serving as a specialised treatment for specific patient populations who cannot achieve adequate cholesterol control through conventional means. This targeted approach aligns with personalised medicine principles while acknowledging the practical realities of healthcare delivery and cost considerations.
Frequently Asked Questions
Is VERVE-102 gene editing safer than taking daily statins?
Currently, statins have decades of safety data in millions of patients and can be stopped if side effects occur. VERVE-102 is still in Phase 1 trials focused on safety, and the genetic changes cannot be easily reversed.
When will gene editing for cholesterol be available to patients?
VERVE-102 is in early Phase 1 trials, meaning years of additional studies are needed before potential clinical use. Even if successful, initial availability would likely be limited to specific high-risk patient populations.
Could gene editing completely replace the need for cholesterol medications?
While gene editing offers the theoretical advantage of permanent cholesterol reduction, it’s more likely to serve as a complementary treatment for specific patients rather than completely replacing proven therapies like statins. Most patients will continue using conventional medications for the foreseeable future.
References
- Cochrane Review: Statins for Primary Prevention of Cardiovascular Disease
- Nature Medicine: VERVE-102 Clinical Trial Results
- Australian Therapeutic Goods Administration: Medicine Approvals
To compare risks directly, link to long‑term safety analyses that underpin statins’ first‑line status, statin safety data.
To put LDL reductions into population‑level context and absolute risk, CDC heart disease statistics.


