Ninety-three percent of colorectal cancers could be prevented or caught early, but standard schedules treat everyone the same. This article cuts straight to the biology behind screening intervals—how the adenoma-carcinoma sequence, polyp size and bleeding patterns determine test sensitivity—and shows exactly when and why you might need tighter surveillance based on family history, inflammatory bowel disease or genetic syndromes.
Key Takeaways
- Colorectal cancer follows a predictable 10-15 year progression from normal cells to invasive cancer, creating an optimal screening window.
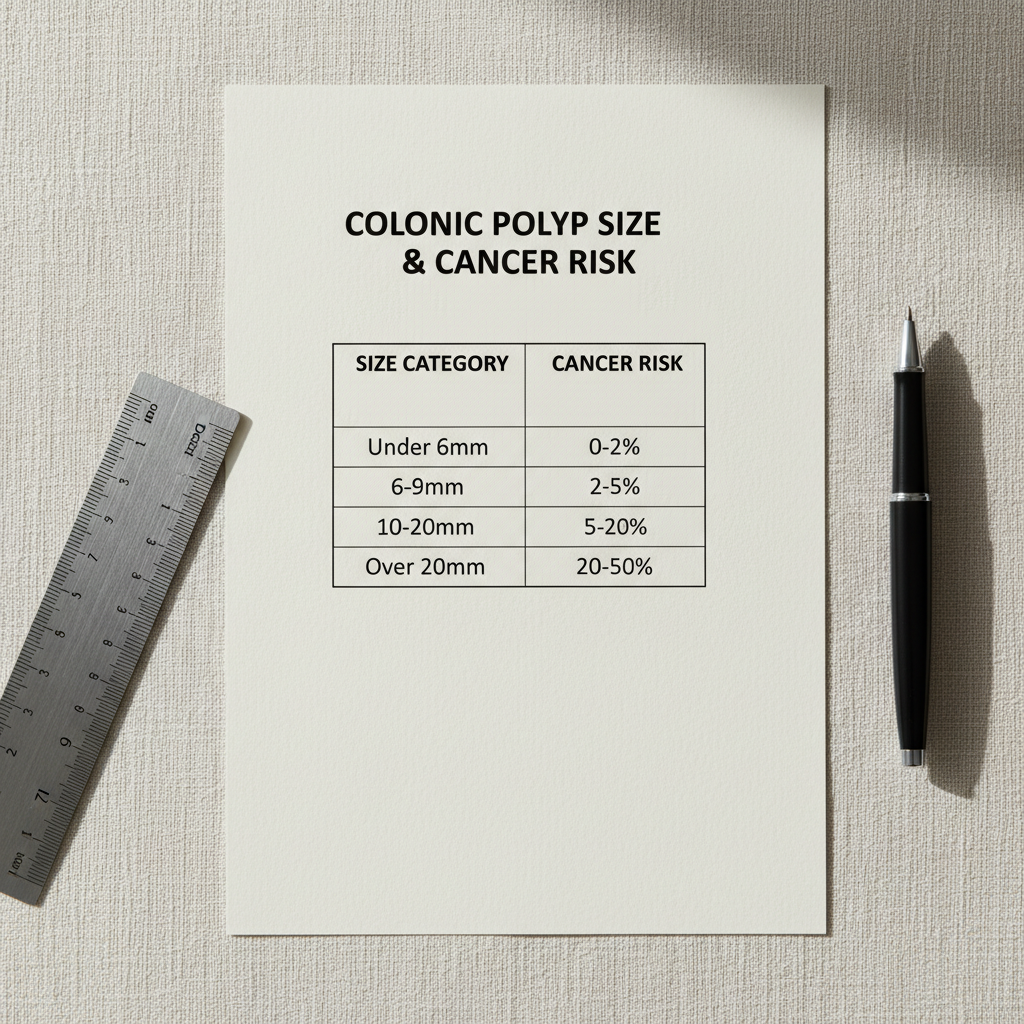
- Polyp size determines cancer risk more than age—polyps over 20mm carry 10-40% malignancy risk compared to less than 1% for polyps under 6mm.
- Your family history, genetic factors, and existing conditions like inflammatory bowel disease require personalised screening schedules beyond standard guidelines.
The 15-Year Journey from Normal Cell to Cancer
Colorectal cancer screening works because of a predictable biological process called the adenoma-carcinoma sequence. Normal cells in your colon don’t suddenly become aggressive cancer—they accumulate genetic mutations over 10 to 15 years before becoming invasive.
This progression starts with small adenomatous polyps, essentially pre-cancerous growths. Most polyps remain small and harmless throughout your lifetime. However, some acquire additional mutations, growing larger and developing more aggressive cellular features. Eventually, a few break through the basement membrane of the colon wall and become invasive cancer.
This extended timeline creates what clinicians call the screening opportunity window. Rather than trying to catch cancer after it forms, screening aims to find and remove high-risk polyps before they ever become malignant.
Why Polyp Size Matters More Than Your Age
The biology of polyp progression reveals why size determines your cancer risk. Small polyps under 6 millimetres carry less than 1% malignancy risk. This explains why gastroenterologists often monitor tiny polyps rather than removing them immediately during colonoscopy.
Polyps larger than 20 millimetres present a dramatically different risk profile, with 10 to 40% cancer probability. The critical target for screening are advanced adenomas—polyps measuring 10 millimetres or larger with high-grade dysplasia or villous features. These lesions are most likely to progress to cancer within 5 to 10 years.
Understanding this biology explains why colonoscopy intervals are set at 10 years after a normal examination. The timing isn’t arbitrary—it’s based on how long new polyps need to develop and progress through the adenoma-carcinoma sequence.
Different Screening Tests, Different Timing
Faecal immunochemical tests (FIT) are recommended every two years because they detect human haemoglobin from bleeding lesions. FIT demonstrates 79 to 88% sensitivity for detecting existing colorectal cancer, but only 23 to 39% sensitivity for advanced adenomas.
This limitation occurs because not all polyps bleed consistently. The two-year testing interval balances early cancer detection while avoiding excessive false positives from benign bleeding sources like haemorrhoids or anal fissures.
Colonoscopy remains the gold standard with 95% sensitivity for cancers and 85 to 95% sensitivity for advanced adenomas. Unlike other screening methods, colonoscopy both detects and removes polyps during the same procedure. This prevention capability justifies the extended 10-year interval between screenings.
When Standard Guidelines Don’t Apply
Your personal biology may not follow standard timelines. If you have inflammatory bowel disease, chronic inflammation accelerates genetic mutations. Your colorectal cancer risk increases 10 to 20-fold, requiring screening every 1 to 2 years after 8 to 10 years of disease duration.
Lynch syndrome carriers have defective DNA mismatch repair genes, developing colorectal cancer with 70 to 80% lifetime probability. These genetic factors compress the normal adenoma-carcinoma timeline, necessitating colonoscopy starting at age 20 to 25, repeated every 1 to 2 years.
Strong family history also alters your risk profile. Having a first-degree relative diagnosed before age 60 triples your baseline risk. Clinical guidelines recommend starting screening 10 years before your relative’s diagnosis age, or at 40—whichever comes first.

The Rising Trend in Young Adults
Colorectal cancer rates in adults aged 20 to 49 have been rising by 1 to 2% annually since the 1990s. This concerning trend prompted discussions about lowering standard screening age recommendations from 50 to 45 years.
The challenge lies in early detection. Seventy-five percent of colorectal cancers are sporadic, occurring without obvious family history or genetic syndromes. Most early-stage colorectal cancers remain completely asymptomatic. When symptoms like bleeding or bowel habit changes finally appear, cancer has often progressed beyond highly treatable early stages.
Optimising Your Personal Screening Strategy
Screening effectiveness depends entirely on adherence to recommended intervals and following up abnormal results. A positive FIT test has only 10 to 15% positive predictive value for cancer, but 40 to 50% for advanced adenomas. The follow-up colonoscopy remains essential regardless of the low cancer probability.
Lifestyle modifications can reduce your colorectal cancer risk by 20 to 40%. Maintaining healthy weight, regular exercise, limiting red meat and processed foods, avoiding smoking, and moderating alcohol consumption all influence the underlying biological processes driving cancer development.
Future screening approaches are moving towards truly personalised medicine. Researchers are developing blood-based tests detecting circulating tumour DNA, artificial intelligence systems improving polyp detection during colonoscopy, and polygenic risk scores to refine individual screening strategies based on your unique genetic profile.
Frequently Asked Questions
How often should I get screened if I have a family history of colorectal cancer?
If you have a first-degree relative diagnosed before age 60, start screening 10 years before their diagnosis age or at 40, whichever comes first. Your screening intervals may be shorter than the standard 10 years, typically every 5 years depending on your specific risk factors.
Can I rely on at-home FIT tests instead of colonoscopy?
FIT tests are effective for initial screening but have limitations—they detect only 23-39% of advanced adenomas compared to colonoscopy’s 85-95% detection rate. Any positive FIT result requires follow-up colonoscopy for complete evaluation.
Why are colorectal cancer rates rising in younger adults?
Rates in 20-49 year-olds have increased 1-2% annually since the 1990s, though the exact causes remain unclear. This trend has prompted discussions about lowering screening age recommendations from 50 to 45 years for average-risk individuals.
https://youtu.be/MB\_agwO4y\_U
References
- Cancer Australia Bowel Cancer Screening Guidelines
- NHMRC Clinical Practice Guidelines for Surveillance Colonoscopy
- Circulating Tumour DNA in Colorectal Cancer Screening Research
For people relying on at‑home testing, a short primer on FIT sensitivity and proper sampling can reduce false negatives and missed advanced adenomas. FIT sensitivity and proper sampling.
Current population‑level screening recommendations and the rationale behind starting age and intervals are summarised in the USPSTF guidance. USPSTF colorectal cancer screening recommendation.
For a clear comparison of test performance (FIT versus colonoscopy) and recommended intervals, reference the American Cancer Society’s screening overview. American Cancer Society screening tests.
The CDC provides concise, patient‑oriented summaries of screening options and follow‑up steps after a positive test. CDC colorectal screening basics.
National surveillance protocols and evidence that inform colonoscopy interval decisions are detailed in Cancer Australia’s clinical guidance. Cancer Australia surveillance guidance.
The biological foundation for these screening intervals comes from decades of adenoma-carcinoma sequence research documenting the 10-15 year progression timeline. adenoma-carcinoma sequence research.
Multiple population studies have documented rising colorectal cancer rates in young adults, prompting recommendations to lower screening age. rising colorectal cancer rates in young adults.